From my formal medical training and every day I provided care to patients, I honed my skills with a singular focus: caring for the person in front of me. I learned how to build trust with patients, understand their health needs, and precisely diagnose and treat any number of health conditions.
As physicians, we are taught that precision, empathy, and individually tailored care define good medicine. But a pandemic that has claimed more than a half-million American lives underscores the inadequacies of a system focused almost exclusively on the medical treatment of individuals. There has never been a more urgent need to integrate public health—the discipline of improving the well-being of whole populations—into patient care and, critically, to take advantage of public health’s focus on confronting community issues that predict our health.
Since the early 1900s, a wide gulf has separated medicine from public health. There are many reasons for this gap, but a clear line can be drawn back to the fall of 1914.
Medical education in the U.S. was undergoing a sweeping transformation as medical schools sought to standardize and bring rigor to physician training. In the process, many began offering postgraduate courses in public health. Disciplines such as disease prevention, epidemiology, and sanitary science were gaining prominence, though their role in patient care was hotly debated.
In this climate, the Rockefeller Foundation convened a fateful October meeting of public health leaders, foundation members, and physicians to envision a modern public health curriculum. The prevailing belief stemming from the conference was that public health would be best distinguished as separate from medical education. This philosophy—with the financial backing of the Rockefellers—would go on to influence some of our nation’s most revered public health schools.
While well-intentioned and warranted in many ways, public health’s break from medicine has come at a high cost.
Practically speaking, medicine and public health have operated in isolation for more than a century, with public health often treated as a second-class discipline. By 1994, only 1% of U.S. physicians had received formal public health training. Public health also remains a fraction of our nation’s nearly $4 trillion health care budget—with funding projected to fall below 2.5% of total spending by 2023.
That is despite well-established evidence that 60% to 70% of the factors that determine our health are social, environmental, and behavioral in nature—issues at the heart of public health practice. And yet our sprawling health care system remains fixated on the treatment of individuals who are sick instead of preventing disease and maintaining health at the community level.
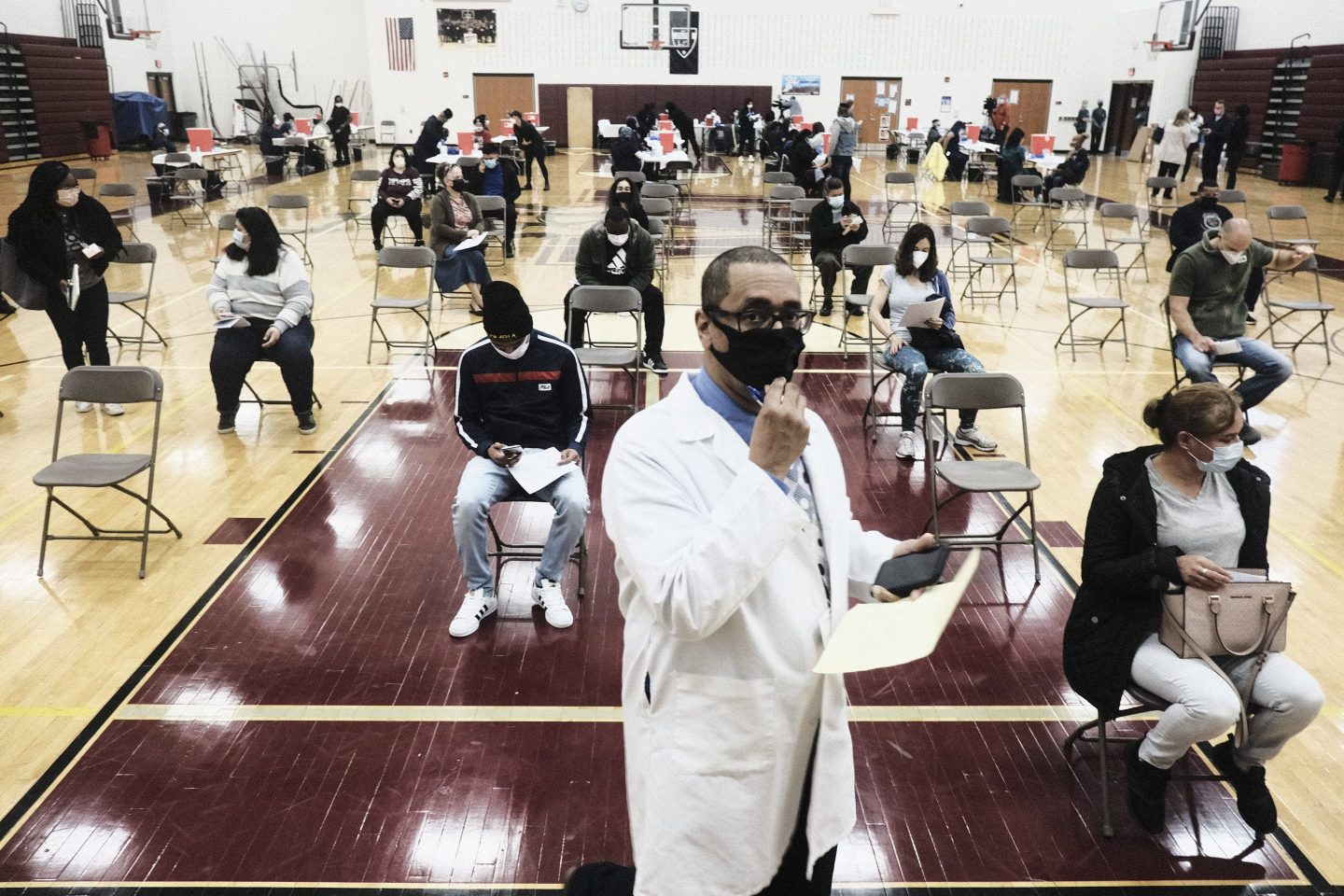
We have seen the ramifications of this system laid bare by COVID-19: glaring racial health inequities, overwhelmed intensive care units, and a national vaccination rollout that launched in fits and starts and continues to encounter public hesitancy.
For two disciplines that have remained far apart, our worlds have suddenly collided, and physicians, in particular, have struggled to engage a health crisis that demands keeping entire populations healthy and out of harm’s way.
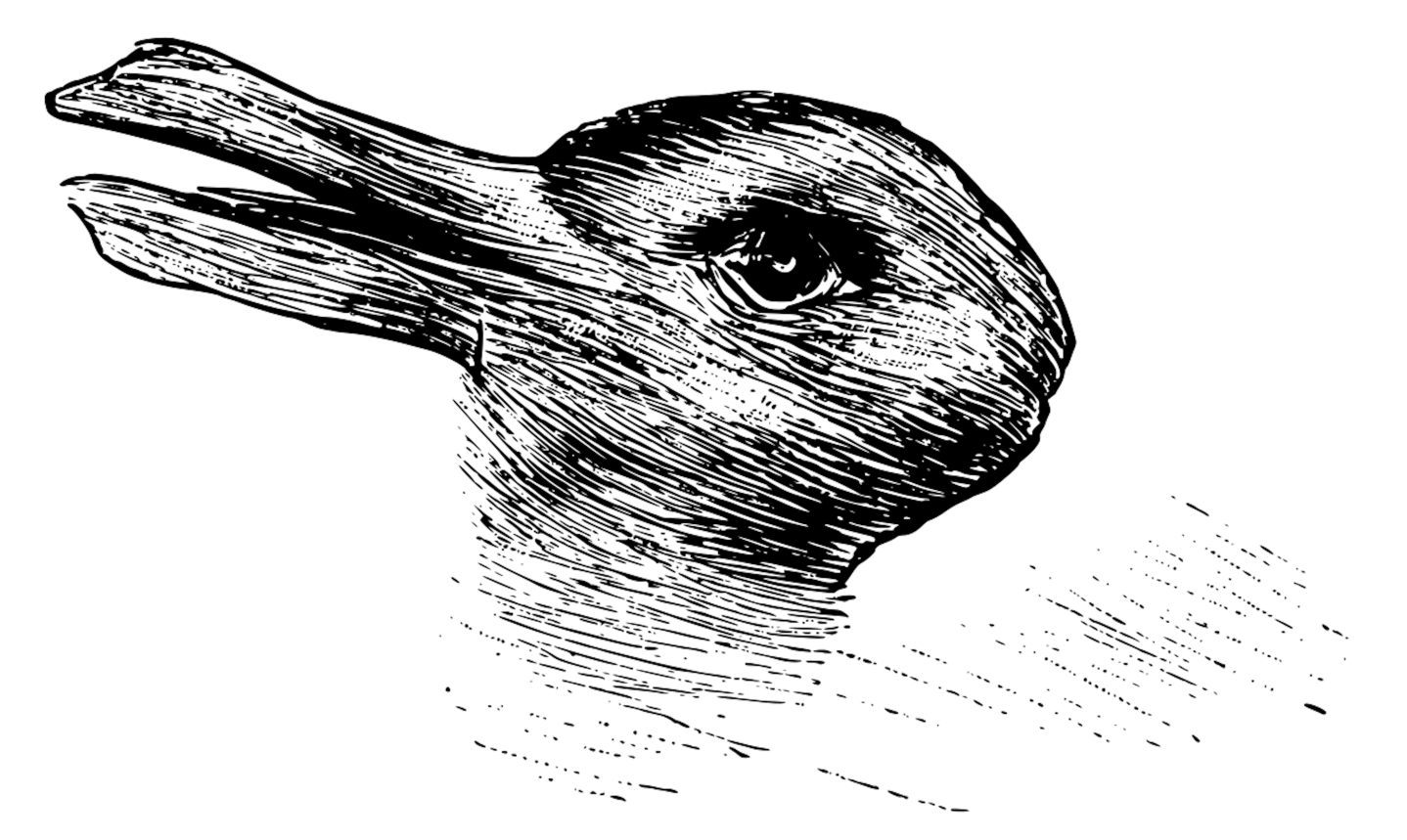
Rabbit, or duck?
This classic illusion captures the problem. When it comes to promoting health, one side sees rabbit, the other sees duck; neither see both simultaneously.
To fundamentally address our health care system’s deficiencies and avoid a repeat of another catastrophic pandemic, we need both perspectives in medicine; public health must become an integral part. To continue behaving as though community health has no bearing on individual health is to believe an illusion. A tree cannot thrive in a burning forest—no more than a patient can expect a long and healthy life in an underserved community with crumbling public health infrastructure.
I am by no means the first to point out this disconnect. Many laudable initiatives have sought to bring the two disciplines together, including a decades-long partnership between the Association of American Medical Colleges and the U.S. Centers for Disease Control and Prevention. What’s different now is that the pandemic has shattered any remaining illusions about medicine’s capabilities. Expert care of patients and biomedical research save lives, but they take us only so far.
While many medical schools, including at Stanford, offer training in public health through dual-degree programs and supplemental coursework, this still puts too much of the onus on medical students to volunteer for these opportunities. Future training must natively integrate public health concepts into the core curricula.
Beyond training, our “sick care” system is still largely a product of our payment system. Reimbursement for public health interventions—the kind that aim to prevent disease—is nonexistent or marginal at best. We cannot expect physicians to practice population medicine without the financial support to do so. Until we have a payment system that rewards for outcomes, we can expect the same results.
Physicians will always concentrate on the patient in front of us. But we let that patient down if we don’t broaden our perspective to see not just an individual but a member of a community. It’s time to give our rabbit and duck problem a hard look.
Lloyd Minor is a scientist, surgeon, and the Carl and Elizabeth Naumann Dean of the Stanford University School of Medicine. He is also the author of Discovering Precision Health.











